By Lynn Razzano RN, MSN, ONCC
(This article was first published in Ob/Gyn.net.)
Every physician knows that venous thromboembolism (VTE) kills. Often, there are symptoms, such as pain and swelling in the leg or a severe headache. If a patient communicates these symptoms to you, there is a good chance that if a VTE is responsible it can be identified and managed. But sometimes, VTE is sudden and has catastrophic results, as it did with Amee VanTassell, pictured left with her father. She died from a blood clot 4 days after delivering her daughter via cesarean section at the age of 36.

Other patients, such as Amber Scott, are luckier. Amber, now age 30 (pictured right with her daughter), fell into a coma because of a blood clot that developed in her brain. While in a coma, a cesarean section was performed, and Amber was delivered of a healthy baby girl. More than a year later, Amber’s recovery from the blood clot that nearly claimed her life continues with daily outpatient rehabilitation sessions.
The good news is that new guidelines for VTE prevention in pregnancy have been released, and incorporating them into your clinical practice should result in minimizing the number of cases of VTE in pregnant patients admitted for delivery or other procedures.
These new guidelines, from the Institute for Healthcare Improvement, the National Perinatal Association, and the Physician-Patient Alliance for Health & Safety, feature recently released recommendations that maximize VTE prevention by detailing the following clinical steps:
- Admission/transfer of care.
- Recommended prophylaxis regimen.
- Patient reassessment.
- Patient discharge.
What are these guidelines?
The guidelines—Ob/Gyn VTE Safety Recommendations for the Prevention of VTE in Maternal Patients—are available in both a checkable version or a pdf format, and were developed with the advice and counsel of a panel of experts brought together by the Physician-Patient Alliance for Health & Safety.
The development of these recommendations included a review of all current peer-reviewed obstetric literature. Since there had been no ideal OB VTE Risk Factor assessment that had scores related to the risk and that quantified the risk severity, the creation of both indexes was needed. In addition, the sequence of clinical steps that would consistently result in a reduction in cases of VTE was identified so that these recommendations would be clinically relevant.
Specifically, the guidelines provide 4 concise steps that direct clinicians to:
1. Assess patients for VTE risk with an easy to use automated scoring system.
2. Provide the recommended prophylaxis regimen, depending on whether the mother is antepartum or postpartum.
3. Reassess the patient every 24 hours or upon the occurrence of a significant event, such as surgery.
4. Ensure that the mother is provided appropriate VTE prevention education upon hospital discharge.
These practice recommendations should be utilized on all obstetric patients entering any healthcare system and offer a much-needed defined process to eliminate OB VTE in clinical practice.
For these recommendations to be most effective, patient engagement, education, and “buy in” along all steps in the continuum of care is key. This “person-centered care” is critical as patients enter our health system and should begin as early as an office visit, which may prompt an ordered procedure. Providing such care should result in a successfully safe patient encounter that achieves maximum VTE and harm prevention, representing a standard of care that maximizes benefits and that all patients are entitled to receive.
In the words of Frank Federico, RPh, Executive Director at the Institute for Healthcare Improvement and member of the Patient Safety Advisory Group at The Joint Commission, “These recommendations focus on prevention measures that can easily be adopted and used by healthcare facilities to prevent VTE and help ensure that delivering mothers go home safely with their babies.”
How can you implement these guidelines?
Physicians can advocate that the hospitals and clinics in which they practice adopt practices and incorporate the guidelines in the facility’s electronic medical record system, setting a standard of care across the health system. An implementation track for using these recommendations on in institution level is set forth below.
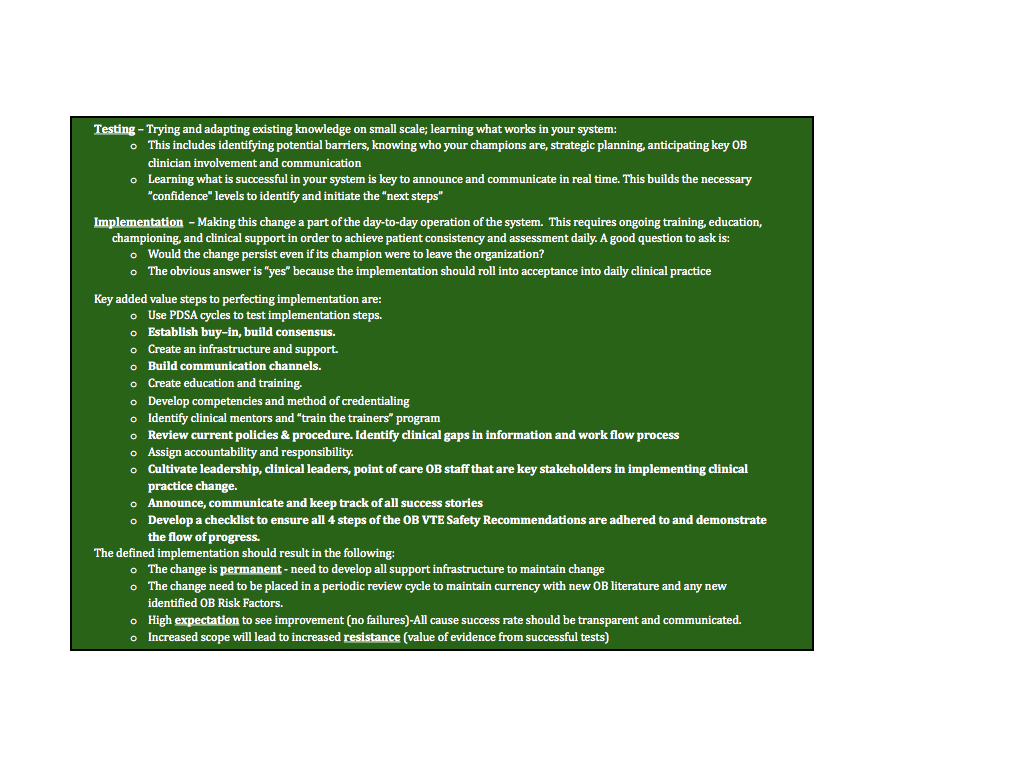 Aside from this broader task of institution-wide implementation, which may be easier in theory, clinicians can commit to advocating for clinical practice change that will help protect their patients from VTE in pregnancy. Outlined below are ways in which you or your department can advocate for adoption of these obstetric VTE prevention guidelines.
Aside from this broader task of institution-wide implementation, which may be easier in theory, clinicians can commit to advocating for clinical practice change that will help protect their patients from VTE in pregnancy. Outlined below are ways in which you or your department can advocate for adoption of these obstetric VTE prevention guidelines.

The time to implement these obstetrical clinical practice changes is now. A second may be too late. Remember that VTE is silent; harm is noisy. Prevention of both is necessary.
I hope those who read this article on OB VTE Safety Recommenadations take the time to review them and incorpoarte into our OB practice. These are an imperative to maximize your OB patient population against the development of VTE and promote ultimate patient safety and harm reduction. I hope you will make comments ont he article and share any experience on your clinical practice. This includes potential barriers or success stories and highly value any clinical comments. Practice change is difficult ,saving patients lives is the true reward. It is never too late to start , it is if a pregnant women succombs as a result of a preventable VTE.
Thanks Lynn Razzano RN, MSN, ONCC
I actually agree with Lynn Razzano. Thanks for the writing up the article though.