Good news and bad news.
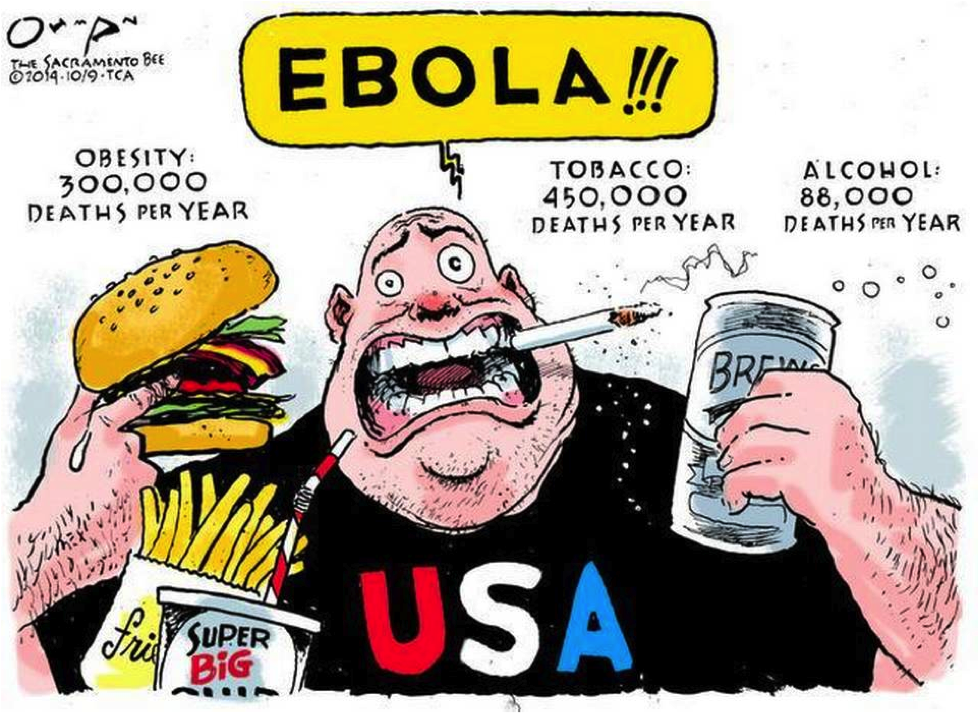
Yes, there have been other things going on in healthcare other than Ebola-mania … thanks @sacbee_news for this illustration putting Ebola in perspective:
The Good News
First, we’ll start with the good news, because most people love a celebration.
In case you missed it, October 29 was World Stroke Day!
As well, in case you may have missed it, to prevent DVT in stroke patients, the recent landmark study Clots 3 led by Martin Dennis, MD (University of Edinburgh, Western General Hospital) needs to be read and followed.
In our interview for Practical Neurology, Dr. Dennis explained how he thinks Clots 3 will change clinical practice:
“CLOTS 3 showed for the first time that thigh-length IPC [intermittent pneumatic compression] reduces the risk of DVT after stroke, and moreover improved survival. Therefore, I would expect its use to increase rapidly. Certainly in the UK there are national programs to introduce IPC into all stroke units; national stroke audits are monitoring its use.
Could better preventive practice have helped prevent blood clots for this North Carolina mother? We would love to hear if you think that the OB VTE Safety Recommendations might have helped, as it did for this obstetric patient.
The Bad News
Not only are liability claims over $2 million against hospitals continuing to rise, but new research suggests that hospitals may be losing the battle to reduce readmissions, and UCSF researchers logged 2.5 million patient alarms in one month.
To top it off, the United States ranks last among wealthy nations in access to healthcare.
Moral of the Story
And, just because a good and bad news story needs a “moral” to the tale…
In this Wall Street Journal article, our own advisory board member, Frank Overdyk, MSEE, MD (Executive Director for Research, North American Partners in Anesthesiology; Professor of Anesthesiology, Hofstra North Shore-LIJ School of Medicine) reminds us:
We can’t always predict when a patient will slip from moderate sedation to deep sedation,” he says, and if the staff is unaware or inexperienced, and help isn’t available to deal with breathing and airway issues, a patient can suffer an oxygen-related brain injury “in approximately five minutes.”
So, the moral of the story – make sure you or your patients are continuously monitored for oxygenation and ventilation when opioids are administered, as recommended recently by the Anesthesia Patient Safety Foundation.