By Sean Power (Community Manager, Physician-Patient Alliance for Health & Safety)
Patients are admitted to some hospitals with an unreported previous diagnosis of obstructive sleep apnea (OSA).
That might be about to change thanks to computer decision support alerts, according to R. Scott Evans, PhD, and a team of researchers at Intermountain Medical Center, a 456-bed teaching hospital in Salt Lake City, Utah.
Dr. Evans presented on the computer decision support alerts in November 2014 at the first meeting of the National Coalition to Promote Continuous Monitoring of Patients on Opioids, which was co-sponsored by the Anesthesia Patient Safety Foundation (APSF), National Patient Safety Foundation (NPSF), The Joint Commission, Premier Safety Institute, and VA National Center for Patient Safety, among others.
The research, although conducted in 2012, was presented at the National Coalition to Promote Continuous Monitoring of Patients on Opioids because conference organizers think his research may contain critical information that should be adopted in the future to improve patient safety. Patients with OSA are still at heightened risk for respiratory compromise, which is the second-most frequently occurring preventable patient safety issue, according to a recent HealthGrades report.
Physician-Patient Alliance for Health and Safety interviewed Dr. Evans about what this could mean for patient safety.
PPAHS: Tell us about obstructive sleep apnea and why you chose to study it.
Evans: Obstructive sleep apnea (OSA) is a condition that interferes with airflow during sleep for anywhere from 2 percent to 14 percent of the population.
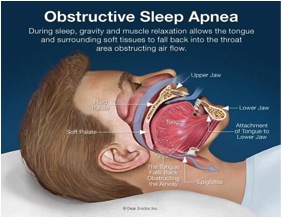
OSA patients are at an increased risk for hypoxemia (low oxygen levels in the blood in the arteries), cardiac arrhythmia (irregular heartbeat), heart failure, stroke and death during hospitalization.
It is a problem, then, when doctors are unaware that their patients experience OSA. Given the risk of OSA-related problems, this can become a significant patient safety issue.

Hospitalized patients with OSA usually receive positive airway pressure (PAP). PAP therapy makes it easier to breathe. When the patient breathes in, the PAP forces air into the lungs, ensuring blood is adequately oxygenated.
When clinicians are unaware that the patient experiences OSA, they are unable to provide appropriate therapy.
It is very important, then, that patients with OSA are identified upon admission so that clinicians have all the information they need to provide the right care.
The problem was that many patients at Intermountain Medical Center had been diagnosed with OSA at other healthcare facilities in the past but the diagnosis was not identified when they were admitted.
PPAHS: What did your team do differently?
As soon as patients were admitted, Intermountain Medical Center checked patient records against a large data warehouse covering a wide geographic area to see if the patient had been diagnosed with OSA in the past.
Clinicians also used screening questionnaires such as STOP BANG to identify hospitalized patients with OSA, especially before surgery.
If the screening process did not identify OSA, their record was checked against the data warehouse to find out if the patient had been diagnosed with OSA by other facilities in the area.

The warehouse systems analyzed patient admissions at various health care facilities and alerted caregivers to previous diagnoses of OSA.
These alerts enabled clinicians to provide the appropriate therapy, thereby decreasing the risk of OSA-related complications.
At Intermountain Medical Center, we continue to use computer decision support alerts and have expanded their use to other hospitals that are part of Intermountain Healthcare.
PPAHS: How was the study designed and what were some of the outcomes?
From January to October 2012, the computer alerts would notify clinicians whether PAP was prescribed; if patients wore a PAP mask at home; and whether their medical history reflected a PAP prescription or recommended oxygen.
The respiratory therapy director and a nurse practitioner from the sleep medicine service would then follow up and documented the respiratory therapy evaluation and patient visits for 500 patients alerted as having previous documentation of OSA.

Of the 500 OSA alerted patients followed by the respiratory director and nurse practitioner for the purpose of the study:
- 141 patients (28 percent) were placed on PAP, 50 of which were requested by respiratory therapy
- 113 patients (23 percent) admitted to having OSA but declined PAP because of discomfort
- 92 patients (18 percent) denied having OSA although they did have previous diagnosis that documented otherwise
- 14 patients (3 percent) were subsequently placed on a ventilator.
PPAHS: What were some of the most notable outcomes?
Evans: Computer alerts resulted in significantly more OSA patients receiving appropriate medical care.
Moreover, significantly fewer experienced hypox