By Laura Menditto, MPH, MBA (Independent Health Outcomes Research Consultant, Laura A Menditto LLC )
What if there existed a way for perioperative nurses to identify patients at high risk of experiencing opioid-related adverse events (ORADEs)? Could hospitals evaluate the potential benefits of targeting high-risk patients for strategies aimed at reducing ORADEs? Could nurses and doctors use the scoring model to predict—and avoid—ORADEs in future patients?
At the annual conference of Association of periOperative Registered Nurses (AORN), which took place March 30 – April 2, 2014, researchers from Memorial Hermann Memorial City Medical Center in Houston, TX, led by Kathy Nipper-Johnson, BSN, RN, CCM (Director of Case Management and Social Services, Memorial Hermann Memorial City Medical Center) presented research seeking to answer these questions. They researched whether it is possible to develop and validate a risk score model to identify patients for pain management strategies.
The risk score model aims at reducing postsurgical ORADEs using hospital administrative data in adults who received opioids following gastro-intestinal (GI) or orthopedic surgeries.
You can download the poster presentation here.
High risk patients lead to more adverse events, longer stays, and greater costs
The researchers analyzed administrative claims data to identify adults who receive opioids following gastro-intestinal or orthopedic surgeries. Using logistic regression, the researchers stratified patients according to risk before applying generalized linear and binomial regression models to compare cost and length of stay (LOS).
The researchers found:
- Of all 4,888 patients analyzed, 551 (11.3 percent) experienced ORADEs;
- Risk factors included age, gender, pre-surgical opioid use, and several comorbidities such as diabetes and obstructive sleep apnea;
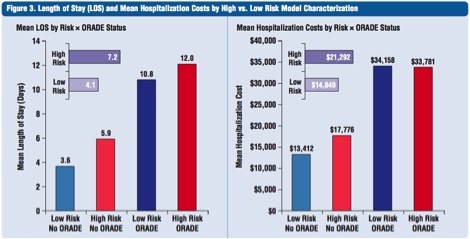
- Higher risk patients stayed longer (7.2 days versus 4.1 days); and,
- It costs more to care for higher risk patients ($21,292 versus $14,849).
Perioperative nurses, suggests the findings, should explore alternative postoperative pain management strategies in higher risk patients. If doing so could decrease ORADE incidence by 25 percent to 100 percent, length of stay could be decreased by 74 to 294 days, and accompanying costs decrease by $255,811 to $1,023,243 per 1,000 patients.

One in four men and three in ten women were classified as high-risk, totaling 29.1 percent of patients. Overall, 22 percent of high-risk patients experienced one or more ORADEs, compared to only 6.9 percent of low-risk patients.
The final composite risk score model effectively predicted specific ORADEs and 30-day readmissions. Of all high-risk patients, 12.3 percent were readmitted within 30 days, compared to 9.1 percent for the low-risk population.

Compared to low-risk patients, high-risk patients tended to have longer LOS (7.2 days versus 4.1 days) and higher hospitalization costs ($21,292 versus $14,849).
Based on these results, alternative pain management strategies intended to decrease ORADE incidence from 25 percent to 100 percent, have the potential to reduce LOS by 74 to 294 days per 1,000 surgical patients, with accompanying savings of $255,811 to $1,023,243.

One size does not fit all when it comes to pain management
Opioids and their related adverse events threaten patient safety, lead to prolonged hospital stays, and increase the economic burden on hospital systems.
By using a risk score model, perioperative teams can identify high-risk patients who are not only pre-disposed to ORADEs based on their risk profile, but who are also more likely to have additional downstream consequences such as longer hospital length of stay, higher readmission rates, and greater hospitalization costs.
Initiatives that target high-risk patients for non-opioid pain management strategies may reduce opioid requirements and prevent these downstream consequences.
Editor’s note: Laura Menditto is a researcher with more than two decades of experience in health economics and outcomes research in the pharmaceutical industry. She received an MPH in 1999 from Drexel University, an MBA in 1995 from Philadelphia University and a BS, cum laude in 1981 from the University of the Sciences in Philadelphia. Ms. Menditto’s work has resulted in more than 40 peer-reviewed presentations at scientific meetings and journal publications. For this project, Ms. Menditto contributed expertise included knowledge of hospital database analyses methods, construction of predictive risk models and writing for scientific meeting presentation and publication.