Presenting at a standing-room-only meeting at the recent International Stroke Conference (ISC), health experts recommended shortened door-to-treatment times and the use of intermittent pneumatic compression (IPC) to help prevent deep vein thrombosis (DVT) and pulmonary embolism (PE) in stroke patients.

Stroke is a leading cause of death and disability in the U.S., with 800,000 cases occurring each year. Each year in the United States, an estimated 300,000 cases of VTE occur. Mortality can be as high as 3.8 percent in patients with DVT and 38.9 percent in those with PE. VTE is associated with a high risk of death in the U.S. and Europe, with an estimated incidence rate of 1 in 1,000 patients. VTE is particularly common after a stroke. Approximately 20 percent of hospitalized immobile stroke patients will develop DVT, and 10 percent a PE.[1]
In reviewing the treatment approaches to prevent DVT in stroke patients, Mark J. Alberts, MD (Clinical Vice-Chair for Department of Neurology and Neurotherapeutics, UT Southwestern Medical Center) spoke about the results of the recent CLOTS 3 study which showed a 29 percent reduction in life-threatening DVT — and a 14 percent reduction in overall mortality — for patients receiving IPC therapy.
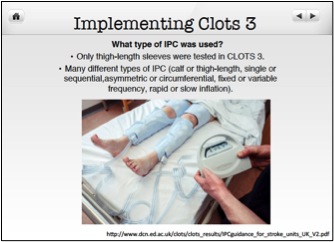
Although there are many different types of IPC (calf or thigh-length, single or sequential, asymmetric or circumferential, fixed or variable frequency, rapid or slow inflation), only thigh-length sleeves were tested in CLOTS 3. Using thigh-length IPC makes intuitive sense, explained Dr. Alberts, as it applies pressure on areas of the leg where blood clots are likely to develop.
Moreover, Dr. Alberts pointed out five key benefits to using thigh-length IPC:
- Non-invasive approach
- Generally well tolerated
- Minimal side effects
- Less costly than medications
- Can be used in all types of stroke patients
Assessing and treating stroke patients should be done in as short a period of time as possible. Successful health outcomes in stroke patients often depends on having as short a door-to-treatment time as possible, emphasized Laurie Paletz, BSN, PHN, RN-BC (Stroke Program Coordinator, Cedars-Sinai Medical Center). Delays in evaluation and initiation of therapy should be avoided because the opportunity for improvement is greater with earlier treatment. This not only means having a collaborative team effort, but looking at anything that might shorten door-to-treatment times, including having designated parking for stroke patients.
Ms. Paletz also highlighted the need to use the treatments that Dr. Alberts discussed. For example, clinicians should make sure that the IPC is being used and not hanging across the bedrail, and that the patient is not only wearing IPC, but that it is turned on.

Unfortunately, the provision of needed prophylaxis has been sub-optimal. Ms. Paletz encouraged clinicians to use available VTE treatments:
Mr. Wong discussed the Stroke VTE Safety Recommendations. These Recommendations may help reduce death and disability among stroke victims due to VTE. Developed by a group of leading neurological health and patient safety experts brought together by the Physician-Patient Alliance for Health & Safety, the Stroke VTE Safety Recommendations incorporate the latest research.
The Stroke VTE Safety Recommendations provide four concise steps that:
- Assess all admitted patients with a stroke or rule out stroke diagnosis for VTE risk with an easy to use checklist.
- Provide the recommended prophylaxis regimen, which includes the use of mechanical prophylaxis and anticoagulant therapy.
- Reassesses the patient every 24 hours, prior to any surgical or procedural intervention or change in the patient’s condition.
- Ensure that the patient is provided appropriate VTE instructions and information upon hospital discharge or transition to rehabilitation.
A pdf of the Stroke VTE Safety Recommendations can be viewed by clicking here.
For a pdf of the presentation given at ISC, please click here.
[1] Dennis MS, Sandercock P, Reid J, et al. Effectiveness of Intermittent Pneumatic Compression in Reduction of Risk of Deep Vein Thrombosis in Patients Who Have Had a Stroke (CLOTS 3): a Multicenter Randomized Controlled Trial. The Lancet. Published online May 31, 2013.