
By Michael Wong, JD (Founder & Executive Director, Physician-Patient Alliance for Health & Safety)
Pediatric Sepsis is a Common and Deadly Problem
According to the Society of Critical Care Medicine (SCCM), pediatric sepsis is a common and deadly public health issue:
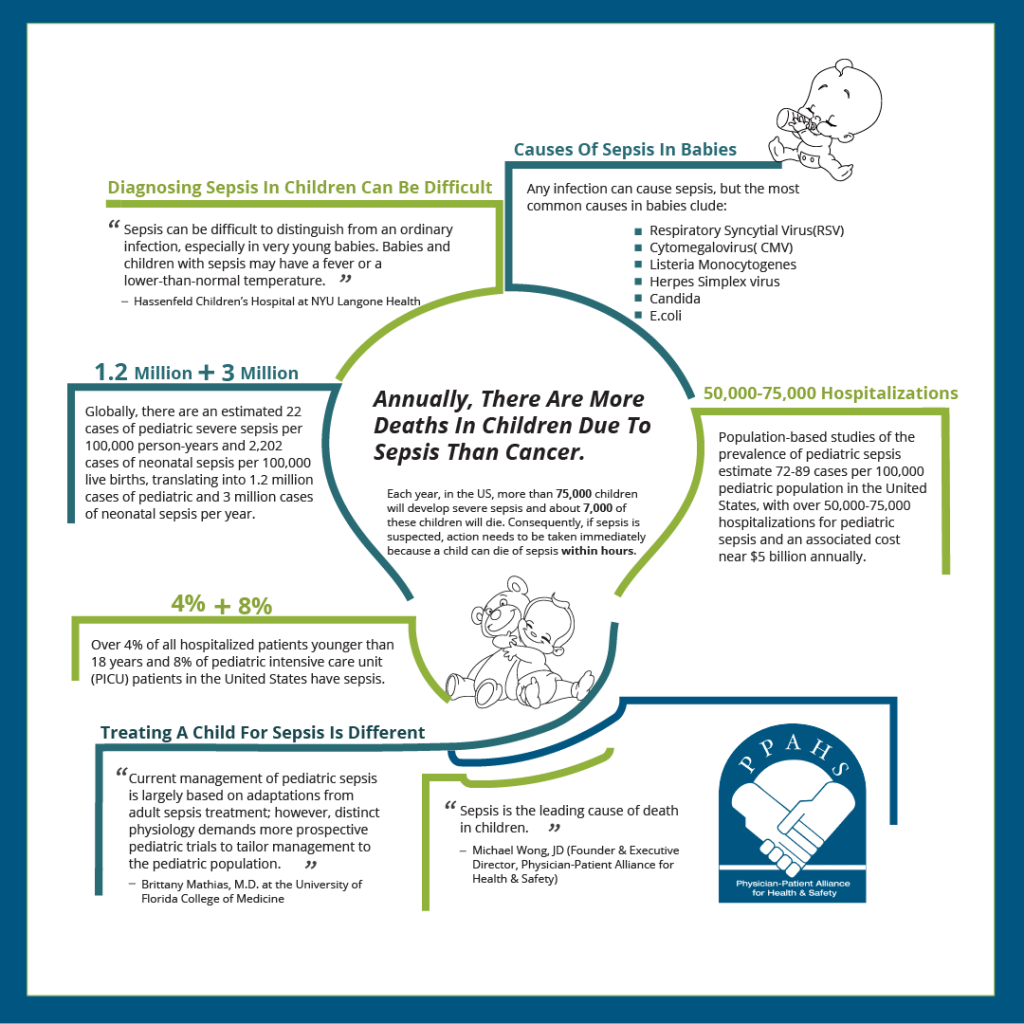
Population-based studies of the prevalence of pediatric sepsis estimate 72-89 cases per 100,000 pediatric population in the United States, with over 50,000-75,000 hospitalizations for pediatric sepsis and an associated cost near $5 billion annually. Globally, there are an estimated 22 cases of pediatric severe sepsis per 100,000 person-years and 2,202 cases of neonatal sepsis per 100,000 live births, translating into 1.2 million cases of pediatric and 3 million cases of neonatal sepsis per year. Over 4% of all hospitalized patients younger than 18 years and 8% of pediatric intensive care unit (PICU) patients in the United States have sepsis. Although estimates are challenged by a lack of standardized data collection and inconsistent reporting, these data confirm that sepsis is common in pediatric patients.

Each year, in the US, more than 75,000 children will develop severe sepsis and about 7,000 of these children will die. Annually, there are more deaths in children due to sepsis than to cancer.
Diagnosing Sepsis in Children can be Difficult
Diagnosing sepsis in children can be difficult. As Hassenfeld Children’s Hospital at NYU Langone Health warns, “Sepsis can be difficult to distinguish from an ordinary infection, especially in very young babies. Babies and children with sepsis may have a fever or a lower-than-normal temperature.”
Consequently, if sepsis is suspected, action needs to be taken immediately because a child can die of sepsis within hours. Healthcare professionals need to quickly recognize the earlier stages of pediatric sepsis, also known as “warm sepsis,” as pediatric sepsis can masquerade as other childhood illnesses.
Treating a Child for Sepsis is Different than Treating an Adult
Children may just be younger in age than adults but treating a child with adult sepsis protocols may not be advisable. As Brittany Mathias, M.D. and her colleagues at the University of Florida College of Medicine concluded:
Current management of pediatric sepsis is largely based on adaptations from adult sepsis treatment; however, distinct physiology demands more prospective pediatric trials to tailor management to the pediatric population.
Fluid Management is Critical for All Sepsis Patients
Fluid management is critical for all sepsis patients but particularly for those in septic shock. For pediatric patients in septic shock, rapid fluid resuscitation is essential and should not be delayed.
However, how much fluid is the question? As Derek S. Wheeler, M.D. and his colleagues at Cincinnati Children’s Hospital Medical Center observe:
Total body water (TBW) as a percentage of body weight decreases rapidly with age. It therefore would be logical to assume that children, due to their relatively greater percentage of TBW, are relatively protected against intravascular volume loss. Unfortunately, this is not the case, primarily because fluid losses are proportionately greater per kilogram of body weight in children versus adults.
As Drs. Niha Peshimam and Simon Nadal (Paediatric Intensive Care, St Mary’s Hospital, London, UK) advise:
All children with septic shock should receive early empiric antimicrobial therapy and aggressive fluid therapy. All emergency departments should have guidelines and protocols in place for the management of sepsis. Sepsis bundles, protocols and guidelines ensure standardised care and have been shown to improve outcome.
These recommendations are echoed by the Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children (2020), which says:
In healthcare systems with availability of intensive care, we suggest administering up to 40–60 mL/kg in bolus fluid (10–20 mL/kg per bolus) over the first hour, titrated to clinical markers of cardiac output and discontinued if signs of fluid overload develop, for the initial resuscitation of children with septic shock or other sepsis-associated organ dysfunction (weak recommendation, low quality of evidence).
In healthcare systems with no availability of intensive care and in the absence of hypotension, we recommend against bolus fluid administration while starting maintenance fluids (strong recommendation, high quality of evidence).
The amount of fluid administered is crucial – with the desired sweet spot being neither too much or too little. Guidance can be taken from four major medical guidelines – SCCM, European Resuscitation Council (ERC), Surviving Sepsis Campaign (SSC), and Pediatric Advanced Life Support (PALS). These major guidelines are all in agreement about the need for and amount of fluids:
- PALS: 20-mL/kg boluses given over 5–10 minutes and titrated to shock reversal.
- ACCM and ERC: 20-mL/kg fluid boluses, up to 40–60 mL/kg for children with signs of inadequate perfusion.
- SSC: 10–20-mL/kg boluses of fluid up to 40–60 mL/kg, with attentive reassessment after each bolus.
Despite these guidelines, Mark Piehl, MD, MPH, and others believe that there is a need for more specific suggestions on the timing, speed, and volume of resuscitation. Given these concerns, healthcare professionals need to exercise their best professional judgment to prescribe treatments that are dependent upon their patient’s individual conditions and medical history.
The Physician-Patient Alliance for Health & Safety (PPAHS) is a proud member of the Global Sepsis Alliance (GSA). Sepsis has impacted PPAHS personally. Dr. Ken Rothfield is Chief Quality & Medical Officer at Texas Health Resources and is on our board of advisors. He developed sepsis following hernia surgery and, consequently, has the unique perspective of knowing sepsis from the point of view of both a doctor and a patient.

We made a podcast with Dr. Rothfield (who was then Chief Medical Officer at Medical City Dallas) in which he discusses his sepsis treatment. Dr. Rothfield emphasizes the need for early detection and treatment of sepsis and implores his colleagues to commit to the early detection and treatment of sepsis:
“I would like you to commit to early detection and treatment of sepsis, because you may not get a second chance to save your patient’s life.
“But, first, you have to know when your patient is suffering from sepsis. You must know at the earliest possible time when sepsis is occurring. Clinical studies show that mortality is significantly reduced if septic patients are identified at early stages of the disease process. In my own case, I was admitting on Thursday, by Friday I was septic, but it was not until Saturday that emergency surgery was performed which removed a section of gangrenous intestine. In my opinion, this can best be done through patient monitoring, which would have been able to provide early detection of my sepsis and I could have had earlier intervention.
“Monitoring a patient’s heart rate and respiratory rate allows clinicians to detect changes over time while supporting hospital protocols for early detection of sepsis. Although nursing assessments taken every few hours may detect sepsis, patient monitoring can alert you at the earliest possible moment when sepsis is developing.
“You may not get a second chance to save your patient’s life – monitor for sepsis.”
For further information on recognizing and treating sepsis in children, please visit the GSA and the Sepsis Alliance websites. With your help, we can achieve early identification and treatment of sepsis in children, and thereby save countless lives.
Michael Wong would like to thank Dr. Amy Campbell, Ph.D., RN, CPHQ, LSBB (Quality Nurse Specialist at Vidant Health in North Carolina) for reviewing this article – although all responsibility for its content and opinion rests with him alone.